Did the Boomers learn to think big when we landed a man on the moon?
AI Overview
Yes, the Apollo program, culminating in landing a man on the moon, certainly spurred a generation, including those born in the post-war baby boom (often referred to as "Boomers"), to think big and pursue ambitious goals. The Space Race and the achievement of putting a human on the moon represented a significant turning point in human history, igniting a sense of possibility and inspiring a culture of innovation and ambition.
Here's why the Apollo program had a lasting impact on the mindset of the Boomer generation:
Technological Optimism:
The Apollo missions, from the launch of the first American satellite Ex1 to the lunar landing, were a testament to human ingenuity and the power of technology to achieve seemingly impossible feats. This fueled a sense of optimism about the future and the belief that ambitious goals were attainable.
Sense of National Pride and Unity:
The Apollo program united the nation behind a common goal and fostered a sense of national pride. The successful lunar landing was a major source of national pride and a symbol of American achievement.
Inspiring Future Generations:
The Apollo missions inspired a new generation to pursue careers in science, technology, engineering, and mathematics (STEM), ultimately leading to advancements in various fields.
Focus on Innovation and Progress:
The program emphasized the importance of innovation and the pursuit of progress. The Boomer generation was raised in a culture that valued technological advancement and a belief that progress was inevitable and desirable.
Example of Human Potential:
The Apollo missions demonstrated that humans are capable of incredible feats when they set their minds to it. This fostered a sense of belief in human potential and the ability to overcome challenges.
In conclusion, the Apollo program served as a powerful catalyst for the Boomer generation to embrace a mindset of "thinking big" and pursuing ambitious goals. It ignited a passion for science, technology, and innovation, and inspired a belief in the potential for human achievement.
Generative AI is experimental.
Higgenbotham's Dark Age Hovel
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
https://www.pewresearch.org/social-tren ... -the-same/Higgenbotham wrote: Sat Apr 26, 2025 1:05 pm Since 1971, the percentage of women who are sole bread winners has more than tripled, from 2 percent to 7 percent. We also know that many, many women now make more than their husbands.
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
Re: Higgenbotham's Dark Age Hovel
https://pierrekorymedicalmusings.com/p/ ... em-failing
DETERIORATING QUALITY OF CARE IN AMERICAN MEDICINE
My next question is whether, in addition to the reasons I gave above for the loss of trust, how much of it is also being driven by a deterioration in the quality of care in U.S hospitals?
I have over 15 years of experience reviewing law firms' medical malpractice cases. In my review of the medical records of Daisy Hillebrand and Kaley Fehr (the two girls in Texas who died of inept medical care, not measles), I found unprecedented missteps, errors, incompetence, and a lack of critical (or clinical) reasoning skills. The abysmal care I witnessed led me to question whether there has been a significant drop in the quality of care in the U.S.
Hypotheses As To Why The Quality Of Medical Care In The U.S Is Deteriorating
1. Widespread Cognitive Impairment In the Wake of the Covid mRNA Campaign (and Covid)
It should be evident that physicians, nurses, and nurse practitioners were among this country's most highly vaccinated subpopulations due to Biden’s Federal CMS mandates.
Just this week, a WSJ article highlighted the “millions of Americans,” both old and young, with new cognitive impairments due to “Long COVID” (which we know from what I bear witness to each day in my vaccine injury and Long COVID specialty practice—it is a euphemism for “Long Vax” - 70+% of my patients' issues started in temporal association with vaccination, not COVID).
In addition, as per AMD, “the COVID vaccines were sold with the most aggressive marketing campaign in history, using healthcare workers as the initial cohort to promote the vaccines since it would be easy to;
1) manipulate them into fully vaccinating
2) have the public trust in their endorsement
3) make them less likely to publicize the side effects of the shots
Because of this, doctors and nurses were some of the most highly vaccinated Americans, and in turn had some of the highest rates of injury.
This is important because cognitive impairment is one of the most common side effects of the COVID vaccines, something not only shown by the data but also in my patients - neurological and cognitive injuries are the rule. The data supporting this reality is overwhelming:
A recent study by Thorpe et al identified alarming increases in 86 adverse events related to brain function, behavior, and cognition following COVID-19 mRNA injection, and another study showed spike protein in the cerebral arteries of vaccinated individuals 17 months out.
AMD’s compilation of data showing the negative cognitive impacts from the mRNA vaccines adds even more disturbing data on the vaccine's impact on cognition.
In a post I wrote about an interview I did with a veteran ER/ICU nurse at The Ohio State University Medical Center (TOSUMC), she reported that many of the illnesses and/or disabilities sufferred by physicians in that system were described to her as being due to neurological issues - either overt neurological deficits or cognitive decline/impairment, and even dementia.
One study published in Nature (one of the top medical journals) reported that after mRNA vaccination, they found a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder.
Another study analyzed individuals over 65 and found Covid vaccination increased the risk of mild cognitive impairment by 138% and the risk of Alzheimer’s by 23%, with smaller increases in vascular dementia and Parkinson’s disease that the authors did not deem to be significant.
VAERS detected a massive spike in cognitive issues being reported to it after the COVID-19 vaccines hit the market.
Ed Dowd has repeatedly documented a significant increase in physical and cognitive disability throughout the adult population, beginning with the onset of the mRNA campaign:
Steve Kirsch was contacted by a whistleblower who reported there had been a 25-fold increase in sudden dementia at the nursing home where she works.
From Igor Chudov’s article on this topic:
I own a small business and deal with many people and other small businesses. Most provide reliable service, remember appointments, follow up on issues, and so on. I noticed that lately, some people have become less cognitively capable. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
Igor Chudov also identified another dataset from the Netherlands, which further corroborated a massive cognitive decline:
The latest quarterly research update from the GOR Network shows that in the first quarter of 2023, there was a 24% increase in GP [general practitioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020.
More specifically, they found:
•No increase was observed in adults under 25 years old.
•A 31% increase was observed in those 24-44.
•A 40% increase was observed in those 45-74 years old.
• An 18% increase was observed in those over 75 years old.
2. Workforce Shortages In The Wake Of The mRNA Campaign
Numerous insurance company reports and studies of actuarial data on the vaccinated report a 37% lower life expectancy and a doubling of the risk of dying. Sun Life Financial’s US operations reported a surge in costly claims that caused stop-loss insurance benefits costs to spike in the fourth quarter.
A new study found massive increases in deaths from Covid-19 in association with increased vaccination among Western Countries by up to 1,275.0%
The Ethical Skeptic analysis of publicly available data finds that cancer diagnoses and expenditures began to skyrocket with the rollout of the mRNA campaign.
The insane number of predominantly young, actively employed Canadian doctors whose deaths have been tracked on social media (132 at last count, two years ago).
In my post on Ohio State University Medical Center, the nurse I interviewed reported that the new cancer center was running out of infusion suites and that cancer surgeries were being delayed due to the excess volume.
Jeff Childers wrote a recent post on cancer clusters reported in numerous and diverse geographic regions, workplaces, and within families. Industrial exposures cannot be blamed given the diversity of cancers and the clustering of different cancers within the same family. The most alarming clusters are occurring among groups of nurses and/or doctors in the same hospital.
More “real-world” evidence of the above comes from my interview with a veteran nurse colleague who has worked at OSUMC for decades. She reported:
An increasingly noticeable number of doctors, nurses, and staff have “died suddenly,” “died unexpectedly,” or have become disabled and ill from injuries and/or cancer. The youth and health of these employees have been increasingly remarked on amongst staff (not to mention the deluge of previously healthy and/or young patients that are now presenting with severe and/or atypical (for that age) illnesses. Remember, cancer used to be a disease of aging essentially.
The suspected role of the vaccines in most of the deaths is an open secret and a growing concern among staff there. Ohio State University Medical Center (OSUMC) stopped emailing out obituaries of prominent or veteran employees when they died. Why do you ask? Because of the uncomfortably noticeable large number of them, which triggered comments by employees openly calling out the likelihood that the vaccines were a cause (i.e., they would point out the dates of the deceased’s vaccination and their death). Unsurprisingly, she also told me that OSUMC would quickly censor any posts of that nature (despite containing no foul language, personal attacks, or threats). From a text conversation we had:
“Yes, this is huge. Lots of internal cases of death and disabilities. They quit posting internal obits for staff. The comments underneath them showed that people knew why everyone was dropping dead for baffling reasons. So those went away.”
Several physicians (the most noticeable of them being super-specialists who cannot be easily replaced), besides dying, were also leaving due to disability or retiring due to unspecified health reasons.
She heard of a growing number of lawsuits by family members of these physicians against OSUMC for the mandates that led to their deaths or disabilities.
One lawsuit was filed by the widow of a physician who dropped dead suddenly. Interestingly, she demanded an autopsy with staining for spike protein, and the heart was found “loaded with spike.”
When physicians die suddenly, this creates a huge mess operationally because “open notes” in the electronic medical record (EMR) can’t be closed, and the chronic, ongoing care of large numbers of often long-time or highly active patients becomes disrupted. In her words, “dealing with the practice of a doc who died is a mess - dealing with open notes, ongoing patient care, patient calls, and maintaining plans of care.”
Many of the disabilities and deaths of physicians were discovered by this nurse while she was following up on notes that were “left open” in the EMR. The staff would then tell her about the injury, death, or disability of the health care provider who started the note. Further, adding the “abandoned” patient panel to healthier and still working physicians in that specialty was causing further strains.
Cancers are exploding at OSUMC, causing massive strain on oncology services, particularly glioblastomas in the brain, as well as in the spine. Also, case managers for many cancer patients stated that they were not retiring due to the volume of patients in need.
Even worse, cancers are being missed at high rates, given that the “index of suspicion” in younger patients is not appropriately high enough. As a result, doctors are missing cancers, as evidenced by retrospectively “obvious” signs and symptoms in the record.
Applications for both short and long-term disability have risen so much that they have created backlogs and delays that staff have noticed and are more openly talking about. The often young ages of the staff applying for disability have not gone unnoticed either.
She knows of several colleagues who are either declining or dying from cancer but are forcing themselves to work to provide for their families.
In a recent conversation with A Midwestern Doctor, they reminded me that we both know numerous doctors who have become impaired or disabled from the COVID vaccines, many of whom then had to enter early retirement, or sadly, died prematurely from a vaccine side effect. Many doctors are still in denial about this.
3. Physician, NP, and Nurse “Burnout” Rates Are Increasing
Physician “burnout” rates increased significantly during the COVID-19 pandemic, from 38.2% in 2020 to 62.8% in 2021. This spike marked an all-time high and ended a previous six-year decline in burnout rates.
4. Attrition Of Physicians From The Workforce
The implications of the rising cognitive issues, deaths, and burnout are that they are leading to an increased physician attrition rate in the United States. Lo and behold:
Job Changes and Retirement: A 2022 survey found that 43% of physicians changed jobs during the pandemic, 8% retired, and 3% left medicine for non-clinical careers—much higher than typical annual turnover rates of 6–7%.
Annual Attrition Trends: Before the pandemic, annual physician turnover increased from 5.3% in 2010 to 7.6% in 2018—a 43% increase. In 2022, 40% of U.S. physicians reported an intention to leave their current job within the next two years. This figure decreased slightly to just over a third (approximately 33–35%) in 2023 but is still historically high.
Specialty and Demographic Variation: The increase in attrition has not been uniform across all specialties or demographics. For example, primary care and rural practice have seen sharp declines in new entrants, and older physicians (65+) are retiring at higher rates.
5. Attrition of Nurses From The Workforce
If you thought the rising attrition rates of doctors were bad, it gets way worse with the nurses. Since the onset of COVID-19, the annual nurse attrition (turnover) rate in the U.S. has also increased significantly. The numbers are eye-popping - multiple studies and workforce reports have documented a sharp rise in both departures and nurses’ intentions to leave the profession.
During the pandemic, about 100,000 registered nurses left the workforce in two years, primarily due to stress, burnout, and retirement.
The psychological impact of the pandemic included increased workload, exposure to critical illness and death, and emotional exhaustion.
**Projections indicate the situation may worsen: If current trends continue, nearly 900,000 RNs (about one-fifth of the U.S. nursing workforce) are expected to leave the profession by 2027.
One-fifth of the U.S. nursing workforce is expected to leave the profession in the next two years? We have to stay out of the hospitals, folks.
6. Increases in “Sentinel Events” Within Hospitals
Based on the above data showing that healthcare providers likely suffered some of the highest rates of cognitive impairment, neurological conditions, cancers, and sudden deaths, which then caused skyrocketing burnout and massive workforce departures, it should come as no surprise that there is a disturbing data trend regarding “sentinel events” in hospitals. First, let’s go over the definition of a sentinel event:
A “sentinel event” is an unexpected occurrence in a healthcare setting that results in:
Death
Permanent harm (e.g., loss of limb or function)
Severe temporary harm (e.g., significant disability or disfigurement)
These events are unrelated to the natural course of the patient’s illness and are often caused by major mistakes or negligence by healthcare providers. Sentinel events are closely investigated by healthcare regulatory authorities to identify root causes and implement corrective actions to prevent similar incidents from occurring in the future.
7. Impacts of Diversity, Equity, and Inclusion Policies
8. The Proliferation Of Lower-Cost, Less Experienced Nurse Practitioners and Physician Assistants
9. Expansion Of Standardized Treatment Protocols At The Expense Of Critical Thinking Skills
Before Covid and my excommunication from the medical system, I loved my career - I was an “intensivist” running ICUs, challenged by the “sickest of the sick,” which required me to find new therapies or approaches when traditional treatments were failing. I was a pioneer in developing and employing specific innovations in my specialty which led me to national and sometimes international acclaim - specifically with the use of therapeutic hypothermia for cardiac arrest, physician performed bedside ultrasonography for rapid identification of organ failure states, and the use of IV vitamin C, thiamine and corticosteroids in sepsis (the Marik protocol).
Beyond that, if someone was in a complete cardiovascular collapse, I could call for emergent infusions of methylene blue, I could use high-dose steroids, I could use Marik’s protocol in non-sepsis conditions, I could use thrombolytics empirically in emergencies, etc.. I did the best I could with often obscured, incomplete, and shifting information as to the actual driver of illness in a crashing patient. I did things without massive randomized controlled trials to support my approach. I could be a “cowboy” when a clinical situation demanded it.
What started to worry me in COVID is that Paul and I would get consulted by family members of severely ill COVID-19 patients who were in a hospital (until we started refusing them due to futility). Over and over we observed cases where the doctors would not “change what they were doing” - they would not try empiric higher dose steroids, not try blood thinners in states of clear hypercoagulability, not add high dose ivermectin in failing cases, not try high-dose IV Vitamin C, not try fluvoxamine or anti-androgen therapy (all beneficial in Covid).
I was shocked that they were sticking to the same lame protocol of low-dose dexamethasone, remdesivir, etc in the face of a deteriorating patient. I could not believe our nation's doctors had stopped doctoring and were instead cowed into submission. It was clear that they were being restricted by heads of hospital committees, pharmacists, and bureaucrats who kept calling for “standardization of treatment approaches” - brazenly oblivious that illnesses and patients are not standardized, as they tend to be more often unique than similar.
I also hypothesize that the weaponized medical boards, societies, and agencies that persecuted outpatient COVID-19 doctors for trying off-label treatments have similarly impacted the psyche of hospital doctors, creating renewed reluctance to treat someone “off-label” or “without sufficient evidence.” I have to admit, though, that the one “bright spot” in the two “measles deaths” is when the doctors decided to treat Daisy with IVIG based on a solid rationale but minimal clinical evidence. So, the spirit for that kind of doctoring still lives, but is becoming rarer, I fear.
I conclude this section with a comment from a reader of the above:
fuzzi: Thorough and relevant. I work with residents and fellows. We have some top notch physicians, and then we have the whiners, complainers, those who can't handle feedback because it's "toxic". Professionalism is lacking, late or no shows to required lectures, scheduled outpatient clinic time, no communication if the resident has decided to not come. Core teaching faculty risk being interrogated by the GME or system higher ups if they try to enforce the rules. One physician told me that he no longer tries to "think outside the box" as he was reprimanded for not following the hospital's protocols. And there's no "right to try". I know a cancer patient who has been doing everything he has been told, whether pharma or chemo or radiation, and nothing is working. He wanted to try Fenbendazole and DMSO, anything at this point because he's dying. The physicians overseeing his treatment won't consider anything because it's not being proven through extensive clinical trials. He's DYING, riddled with cancer, but they're harnessed to protocols and will not consider anything but more of the same useless treatments.
I have lost respect and trust and will be retiring soon. I cannot work with physicians who won't help those who need it most.
10. Corruption And Distortion Of “Evidence-Based Medicine” and The Religious Adherence To Randomized Controlled Trial Data.
“Thou shalt not bow down thyself to them, nor serve them: for I the LORD thy God am a jealous God, visiting the iniquity of the fathers upon the children unto the third and fourth generation of them that hate me; - Exodus 20:5
Re: Higgenbotham's Dark Age Hovel
Much worse than that H.
The hackable human cults have been in the next phase.
The hackable human cults have been in the next phase.
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
https://www.gmo.com/globalassets/articl ... f_3-25.pdf
He was on with Nate Hagens discussing this awhile back.
viewtopic.php?p=87659#p87659
He was on with Nate Hagens discussing this awhile back.
One thing that is concerning is how pervasive these pollutants are. This is not your great great great great, etc., grandfather's collapse.World population is thus likely to be far lower than the 10 billion+ currently projected by
2100. 6 or 7 billion seems far more likely, and if this trend continues further, it could be
down to only 2 or 3 billion by 2200.
viewtopic.php?p=87659#p87659
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
Higgenbotham wrote: Sat Mar 29, 2025 8:57 pm It doesn't seem like the environment is anywhere close to peak microplastics (or nanoplastics, which are smaller). Even if plastic production were to be shut down, it seems existing plastic would still be degrading to smaller particles.
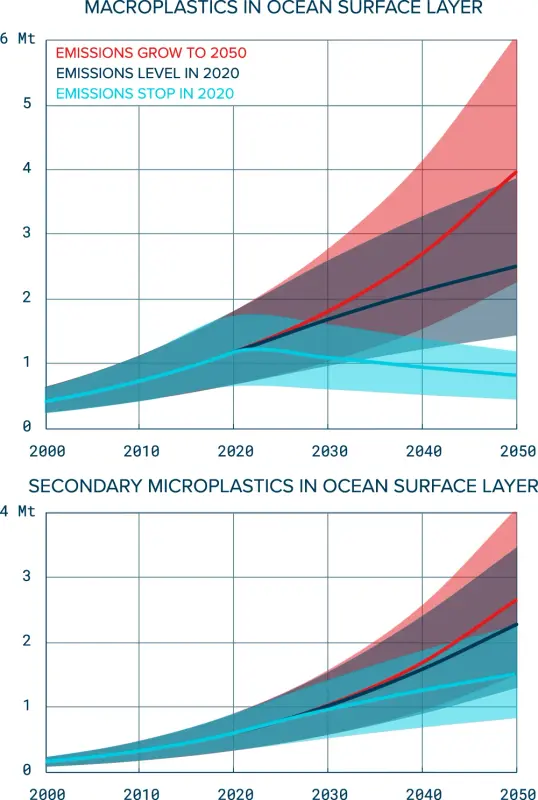
https://www.nature.com/articles/s41598- ... /figures/6
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
Higgenbotham wrote: Sat Mar 08, 2025 8:36 pm My expectation is that as the new dark age tightens its grip, Trump will be spending more and more of his time fighting the crisis or distraction du jour, whether it be the next financial crisis, pandemic, wildfire, measles outbreak, etc., etc., and any grand plans will fall by the wayside and be forgotten.
https://apnews.com/article/kilmar-abreg ... 55420b59eeThe Trump administration appealed. But a federal appeals court backed Xinis’ order for information in a blistering ruling. The case is ongoing.
Meanwhile, President Donald Trump acknowledged to ABC News on Tuesday that he could call El Salvador’s president and have Abrego Garcia sent back.
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
Re: Higgenbotham's Dark Age Hovel
Treasury Department's daily reports on accounts shows the largest rising costs are direct payments to the military and seniors.
We noted a seven percent increase as the keynesian veil moves forward.
The government's ability to borrow using extraordinary measures will probably be exhausted in August or September.
The rot has not even begun to stop. Managed decline as warned since NATA. Decieved...
We noted a seven percent increase as the keynesian veil moves forward.
The government's ability to borrow using extraordinary measures will probably be exhausted in August or September.
The rot has not even begun to stop. Managed decline as warned since NATA. Decieved...
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
There was a test of precipitation extremes over about a 16 hour period ending this morning. While there was flooding in the yard, the pits were able to absorb about 3 inches of rain without showing any standing water after the downpour ended. There's no rain in the 10 day forecast so this could be the heaviest downpour this year. Some future years will probably be worse but, now that this test has passed, it seems OK to expand the garden in the same way it has been done so far.Higgenbotham wrote: Sat Mar 29, 2025 9:24 pm But what I can say is that there seem to be indications, despite the natural tendency of people affected by the weather to complain about it, that growing food has become more difficult. There's been news that that is happening with tomatoes, coffee and cocoa on a worldwide basis now. I'm working hard to make adaptations to that, to become resilient to weather extremes in both temperature and precipitation. My goal in designing these pits was to be able to handle a 4 inch or so 12 hour or so rain without flooding them and to hold that water for the dry periods. Also to be able to carry a heat resistant tomato variety through 95 degree heat and still produce. We should see some tests of that in the next 4 months and I'll talk about it once these extremes are seen.


It can already be said that the experiment with the 12 plants failed. That was to plant in native, unimproved soil. While the 12 plants look healthy, their growth is lagging way behind and they don't show any signs of being able to yield much.Higgenbotham wrote: Sat Mar 29, 2025 7:28 pm We have 6 pits being used for tomatoes with a total of 18 plants. Also 12 of the same plants in a different location as an experiment.
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
-
Higgenbotham
- Posts: 8294
- Joined: Wed Sep 24, 2008 11:28 pm
Re: Higgenbotham's Dark Age Hovel
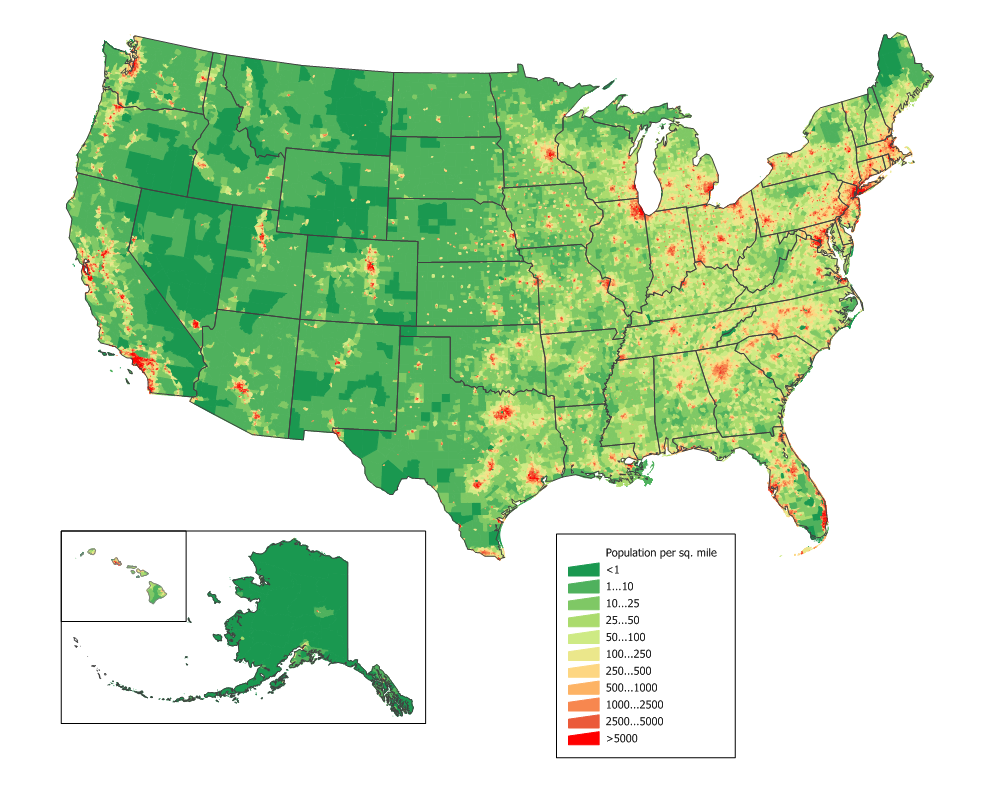
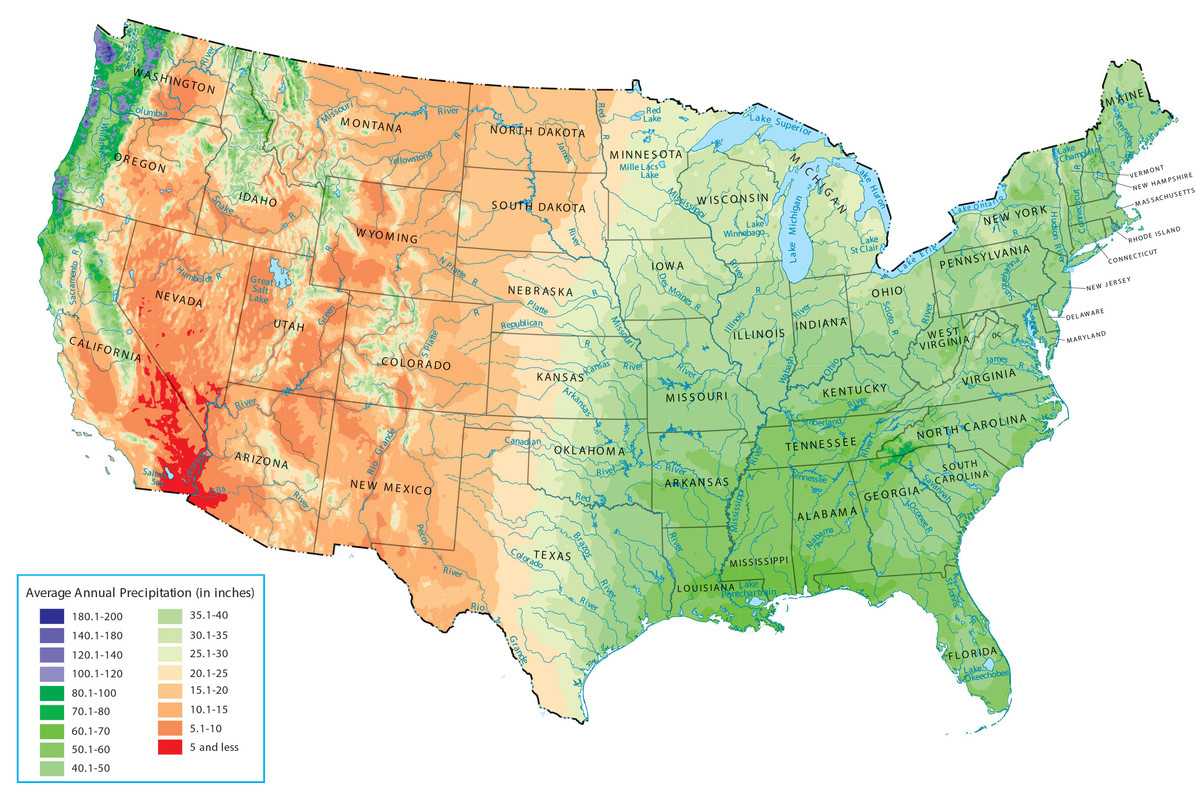
In not too long, this area (Central Texas) will move into the hot, dry season. I want to take advantage of the Spring rains to carry through this season, partly with what these pits absorb and partly with water storage. I am storing some water that I am catching from the roof, but not a lot yet.Higgenbotham wrote: Sat Aug 05, 2023 11:30 am As far as the location for a dark age hovel, my personal preference is the parts of the country where precipitation averages 25-30 inches per year and population densities are lower than near the dark age hovels previously shown. Population density maps align with precipitation maps for the most part. I could get into a long discussion about water but will just use the words personal preference and leave it at that. I'd rather fight water problems than population problems at this time. Also, there are differences where it's very cold and growing seasons are shorter.
With what I have learned over the past year, so far I would rate this area as challenging for survival, but not too challenging. The ground was faster to prep than it would be in colder climates. Once we reach 95 degrees plus for several weeks, I'll report back on how that goes.
While the periphery breaks down rather slowly at first, the capital cities of the hegemon should collapse suddenly and violently.
Who is online
Users browsing this forum: Bing [Bot] and 1 guest